Want to experience the greatest in board studying? Check out our interactive question bank podcast- the FIRST of its kind here: emrapidbombs.supercast.com
Author: Blake Briggs, MD
Objectives: alright so this one should be quick. We will cover priapism, why its bad, ischemic/nonischemic presentation and how to tell the difference, and acute management in the ED.
Priapism: >4 hours of erection.
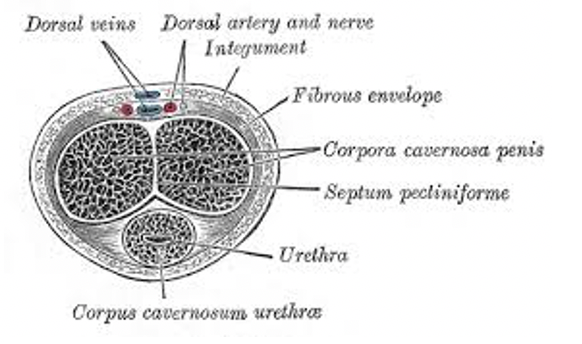
Relevant pathophysiology: erection comes from dilation of cavernosal arteries and decreased venous outflow in corpora cavernosa.
Most common cause: Primary (idiopathic). Super helpful.
Secondary (in order):
Medications- intracavernosal injections, anticoagulants, PDE5 inhibitors, alpha blockers, methylphenidate, cocaine
Any hyperviscosity syndrome (SCD, leukemia, myeloma, etc.)
Diabetes, hyperlipidemia
Pelvic/penile trauma
Some other random ones that won’t be tested or are zebras (…amyloid…)
Two types of priapism: ischemic and non-ischemic
Ischemic = low flow/anoxic/veno-occlusive/time-to-lose-your-penis condition. Medical emergency!
Nonischemic priapism = high flow condition. Nonemergent. Due to high flow into corpora cavernosa. Blood is well-oxygenated.

Sickle cell disease
-known for recurrent priapism that are short episodes but can resolve on their own (“Stuttering priapism”). Can lead to worse ones.
-often associated with awakening from sleep with an erection. Treat them the same as ischemic patients. Make sure they are on Hydroxyurea.
How to manage priapism:
1. Questions to ask patients: duration of erection, prior episodes, if so what was done, medications, illicit drugs, history of SCD, trauma/recent sexual intercourse.
Give these people generous pain meds before sticking needles anywhere.
2. Blood gas analysis: get a 21G needle and aspirate from one side of the corpus, 5 mL.
Ischemic = black blood. Hypoxemia. pH <7.2, high CO2, low O2
Nonischemic = red blood. Normal blood gas.
You can also do Doppler if unable to do blood gas. Low/no pulse for ischemic priapism (#obvi)
3. Let’s begin by saying there are no RCTs or real research behind this stuff. Makes sense really- can you imagine recruiting participants for this sorta thing? “Wait you’re going to stick a needle in my WHAT? Hell nah”
Ischemic treatment:
<4 hours = Intracavernosal phenylephrine injection
>4 hours = Intracavernosal aspiration with/without saline irrigation, with phenylephrine injection
Consider a penile ring block: 25 or 27g needle inserted at penile base on dorsal aspect (see above x-section).
20G butterfly needle – aspirate 5mL from corpora to decompress it – wait 3-5 minutes for response- if none, inject Phenylephrine every 3-5 minutes until resolution or until UP TO 1 HOUR before deciding if treatment is working or not.
Ok so that failed? Call urology (probably should have already). Shunt surgery- fistula made to drain blood.
Avoid: beta-adrenergic agonists, mixed alpha/beta agonists. These can cause smooth muscle dilation.
References
1. Broderick GA, Gordon D, Hypolite J, Levin RM. Anoxia and corporal smooth muscle dysfunction: a model for ischemic priapism. J Urol 1994; 151:259
2. Burnett AL, Anele UA, Derogatis LR. Priapism Impact Profile Questionnaire: Development and Initial Validation. Urology 2015; 85:1376
3. Burnett AL, Bivalacqua TJ. Priapism: current principles and practice. Urol Clin North Am 2007; 34:631
4. Burnett AL. Nitric oxide in the penis–science and therapeutic implications from erectile dysfunction to priapism. J Sex Med 2006; 3:578.
5. Dittrich A, Albrecht K, Bar-Moshe O, Vandendris M. Treatment of pharmacological priapism with phenylephrine. J Urol 1991; 146:323.
6. Moon DG, Lee DS, Kim JJ. Altered contractile response of penis under hypoxia with metabolic acidosis. Int J Impot Res 1999; 11:265.
7. Montague DK, Jarow J, Broderick GA, et al. American Urological Association guideline on the management of priapism. J Urol 2003; 170:1318.
8. Palese MA, Ferrer F, Perlman E, Gearhart JP. Metanephric stromal tumor: a rare benign pediatric renal mass. Urology 2001; 58:462.
9. Pryor J, Akkus E, Alter G, et al. Priapism. J Sex Med 2004; 1:116.
10. Rees RW, Kalsi J, Minhas S, et al. The management of low-flow priapism with the immediate insertion of a penile prosthesis. BJU Int 2002; 90:893.
11. Spycher MA, Hauri D. The ultrastructure of the erectile tissue in priapism. J Urol 1986; 135:142.


