Want to experience the greatest in board studying? Check out our interactive question bank podcast- the FIRST of its kind here: emrapidbombs.supercast.com
Author: Siena Hapig-Ward, MS4; Blake Briggs MD; Mary Claire O’Brien, MD
Introduction
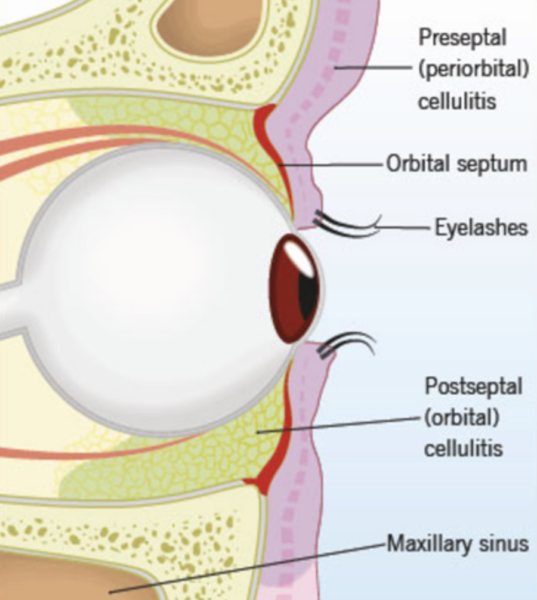
Orbital and preseptal (or periorbital) cellulitis are both infections of the orbital tissues; it is vital to diagnose orbital cellulitis accurately and quickly- it’s a medical emergency. Orbital cellulitis involves the fat and extraocular muscles of the orbit. Preseptal cellulitis involves the tissue anterior to the eye septum, a thin fibrous layer arising from the periosteum along the superior and inferior orbital rims. Neither involves the globe, and preseptal cellulitis does not typically transform into orbital cellulitis.
Pathogenesis
The orbit is surrounded by 3 paranasal sinuses – frontal (superior), ethmoid (medial), and maxillary (inferior) (see image 1).
The #1 cause of orbital cellulitis is ethmoid sinusitis due to the many perforating nerves and blood vessels that enter the orbit. In fact, rhinosinusitis is present in 86-98% of cases of orbital cellulitis.1-4 Other causes include ophthalmic surgery, trauma, infection of teeth/middle ear/face, infected mucocele, or endogenous bloodstream seeding.5,6
What bugs are involved? Unfortunately, it’s often hard to identify.
- Bacterial – Staphylococcus aureus and streptococci species are most common.1-3,8 Prior to the widespread use of the HIB vaccine, Haemophelu influenza B was a common cause.
- Fungi and mycobacteria – Mucorales and Aspergillus should be suspected in immunocompromised patients or diabetics. Usually, these present in a dramatic
fashion, with pain out of proportion on exam.
Presentation
Both preseptal and orbital cellulitis cause ocular pain and eyelid swelling with erythema.
However, ocular cellulitis may ALSO cause pain with eye movements +/- proptosis, ophthalmoplegia, chemosis, decreased visual acuity, fever.1-4,9,10
Be aware that there are many associated complications:7
- Subperiosteal, orbital, or brain abscess
- Epidural or subdural empyema
- Meningitis
- Cavernous or dural sinus thrombosis
- Vision loss can occur in 3-11% of patients, and death in 1-2% of patients, but data is limited11,12
You get the picture. That’s a lot of complications- none of which you need to remember. Just know bad things happen if this infection isn’t properly treated.
While a complete physical exam should be performed, ensure you immediately assess visual acuity and pupillary light reflex, as a sluggish or absent light reflex indicates optic nerve involvement, and complications are prone to develop rapidly.
Diagnosis
While you suspect orbital cellulitis clinically, it is essential to quickly obtain a CT orbit with IV contrast to evaluate for any complications like we listed above (e.g., abscess, empyema, etc).
Without complications, it will likely show evidence of rhinosinusitis, as well as inflammation of extraocular muscles, fat stranding, and anterior displacement of the globe.
Orbital Cellulitis Treatment
Vancomycin 15-20 mg/kg IV BID PLUS ceftriaxone IV OR cefotaxime IV.
If intracranial involvement cannot be excluded or patients have associated chronic sinusitis or odontogenic source, add metronidazole 500mg IV for anaerobic coverage.
If the patient has diabetes mellitus or is immunocompromised and looks unwell or has a complication noted above, add amphotericin 0.3 mg/kg/day IV for fungal coverage.
Disposition
All patients with orbital cellulitis should be seen emergently with ophthalmology consult; additionally, ENT should be consulted if rhinosinusitis is present.
Patients with preseptal cellulitis can be discharged with antibiotic prescriptions and instructions to follow up with their primary care physician. They need to return if they have any fever, changes in vision, or pain with eye movement.
References
- Botting AM, McIntosh D, Mahadevan M. Paediatric pre- and post-septal peri-orbital infections are different diseases. A retrospective review of 262 cases. Int J Pediatr Otorhinolaryngol 2008; 72:377.
- Seltz LB, Smith J, Durairaj VD, et al. Microbiology and antibiotic management of orbital cellulitis. Pediatrics 2011; 127:e566.
- Nageswaran S, Woods CR, Benjamin DK Jr, et al. Orbital cellulitis in children. Pediatr Infect Dis J 2006; 25:695.
- Sobol SE, Marchand J, Tewfik TL, et al. Orbital complications of sinusitis in children. J Otolaryngol 2002; 31:131.
- Weakley DR. Orbital cellulitis complicating strabismus surgery: a case report and review of the literature. Ann Ophthalmol 1991; 23:454.
- Muthukrishnan Vallinayagam, Juhi Sahu, Srikanth Krishnagopal, N Vasantha Kumar. Endogenous orbital cellulitis with optic neuropathy secondary to an intramuscular abscess in poorly controlled diabetes mellitus. J Ophthalmic Sci Res 2019; 57:319.
- Goytia VK, Giannoni CM, Edwards MS. Intraorbital and intracranial extension of sinusitis: comparative morbidity. J Pediatr 2011; 158:486.
- McKinley SH, Yen MT, Miller AM, Yen KG. Microbiology of pediatric orbital cellulitis. Am J Ophthalmol 2007; 144:497.
- Durand, ML. Periocular infections. In: Principles and Practice of Infectious Diseases, 7th ed, Mandell, GL, Bennett, JE, Dolin, R (Eds), Churchill Livingstone Elsevier, Philadelphia 2010. p.1569.
- Rudloe TF, Harper MB, Prabhu SP, et al. Acute periorbital infections: who needs emergent imaging? Pediatrics 2010; 125:e719.
- Osguthorpe JD, Hochman M. Inflammatory sinus diseases affecting the orbit. Otolaryngol Clin North Am 1993; 26:657.
- Erickson BP, Lee WW. Orbital Cellulitis and Subperiosteal Abscess: A 5-year Outcomes Analysis. Orbit 2015; 34:115.
- Scottish Antimicrobial Prescribing Group. “Orbital Cellulitis”. https://www.antimicrobialcompanion.scot/nhs-lothian/body-systems/skin-and-soft-tissue-infections/orbital-cellulitis/



