Want to experience the greatest in board studying? Check out our interactive question bank podcast- the FIRST of its kind here: emrapidbombs.supercast.com
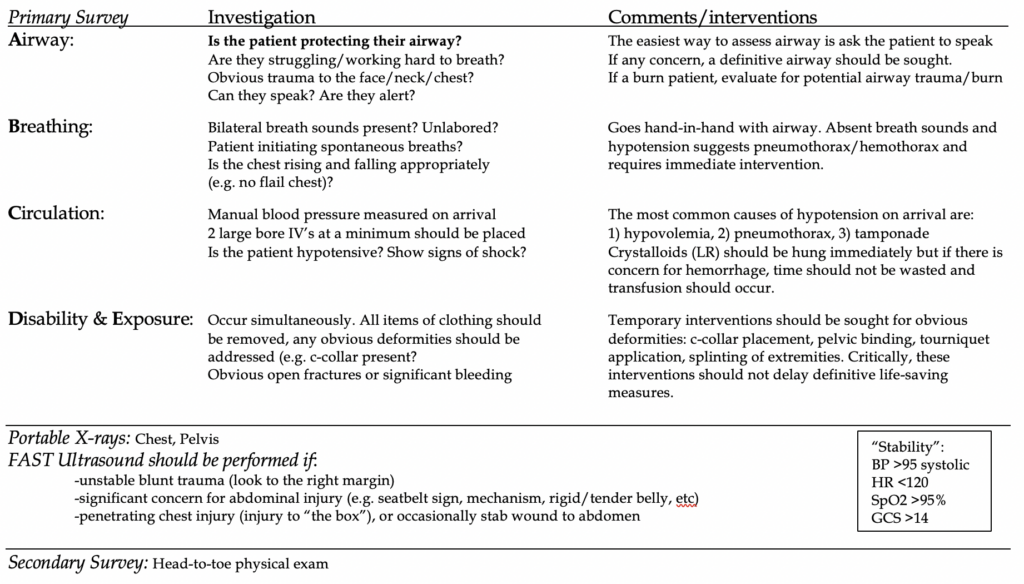
Objectives: define blunt versus penetrating trauma, understand the critical points of the primary survey, indications for FAST, highlight the secondary survey, disposition of trauma patients
Disclaimer: this guide will provide a generalized overview and approach to understanding the evaluation of patients of trauma. This does NOT serve as an all-encompassing guide and does not account for the variable presentations. As is often said, patients do not read the textbook.
Blunt trauma: most common overall cause of trauma in the United States. ~75% are from MVCs.
Blunt forces push against the anterior thorax and abdomen, compressing viscera against the posterior thoracic cage or vertebra, causing crushing of tissue and shearing open organs at their point of attachment to the peritoneum. Spleen and liver are most commonly injured in the abdomen in blunt trauma. Retroperitoneal structures are also at risk. Tears or stretch injuries to arteries, can result in infarction downstream tissues. The kidney is most susceptible to such stretch injury.
Quick hits:
Bike handlebar injury: duodenal rupture, pancreatitis
Lap belt injury: small bowel rupture
To assess pelvic fractures, gentle lateral compression of iliac wings is all that is needed
Sternal fracture is associated with aortic injury in <10% of patients. Rib fracture is the most common associated fracture
Penetrating trauma: any object that breaks the skin barrier and enters or “penetrates” the body at a particular location. The most common cause is a tight heat between ballistic injury and stabbing. Other causes include various work-related or random hazards. In general, ballistic injury causes more damage due to force principle alone and will more often than not require operative intervention due to concern for pressure-wave damage to nearby structures.
Quick hits:
GSW to abdomen: 80% mortality, most common location is small bowel
Stab wound to abdomen: 20% mortality, most common location is liver
In order of most likely damaged organs in penetrating trauma to the abdomen: small bowel > liver > colon
Most common injury in the chest is a pneumothorax, followed by pulmonary contusion, hemothorax, tamponade, tracheobronchial injury.
References:
· Davis JJ, Cohn I Jr, Nance FC. Diagnosis and management of blunt abdominal trauma. Ann Surg 1976; 183:672.
· Greaves, I. Porter, K. Garner, J. (2009). Trauma Care Manual 2nd Ed. London: Hodder Arnold.
· Hunt, P. Greaves, I. & Owens, W. (2006). Emergency thoracotomy in thoracic trauma-a review. Injury. 37, 1-19. PMID: 16410079
· Isenhour JL, Marx J. Advances in abdominal trauma. Emerg Med Clin North Am. 2007 Aug;25(3):713-33, ix. Review. PubMed PMID: 17826214.
· Lent, G. & Kumar, N. (2009). Emergency Bedside Thoracotomy. emedicine.com
· Meredith, W. & Hoth, J. (2007). Thoracic Trauma: When and How to Intervene. Surgical Clinics of North America. 87, 95-118. PMID: 17127125
· Van Waes OJ(1), Van Riet PA, Van Lieshout EM, Hartog DD. Immediate thoracotomy for penetrating injuries: ten years’ experience at a Dutch level I trauma center. Eur J Trauma Emerg Surg. 2012 Oct;38(5):543-51. doi: 10.1007/s00068-012-0198-6. Epub 2012 Jun 16.



