Want to experience the greatest in board studying? Check out our interactive question bank podcast- the FIRST of its kind here: emrapidbombs.supercast.com
Author: Blake Briggs, MD
Introduction
Board exams occasionally test on evidence-based medicine pathways, especially ones in emergency medicine that reduce cost to the patient and their exposure to radiation. This rapidly reviews the evidence-based medicine behind the process of clearing a cervical spine and discussing the need for imaging in the setting of stable, minor blunt trauma patients.
Background
For any patient with a possible cervical spine injury, it is still standard of practice to initiate spinal immobilization. The conservative approach is to assume the possibility of a cervical spine injury in any patient; however spinal immobilization has its own risks and adverse effects long term. We get it. We personally aren’t the biggest fans of cervical collars in awake and alert patients, but the boards want you to be conservative! In unstable trauma patients requiring immediate surgery, cervical collar should be maintained and cleared later after life-threatening injuries have been dealt with. In those with major trauma undergoing CT imaging of the head, chest, abdomen or pelvis, CT cervical spine should be obtained as well.
The following determines who is high risk and likely requires empiric C-spine imaging (these patients will likely already be receiving other CT scans):
– High speed motor vehicle crash (≥35 mph)
– Death at the scene of motor vehicle crash
– Fall from height ≥10 feet
– Significant intracranial injury and/or skull fracture on CT head
– Neurologic symptoms or signs
– Pelvic fractures
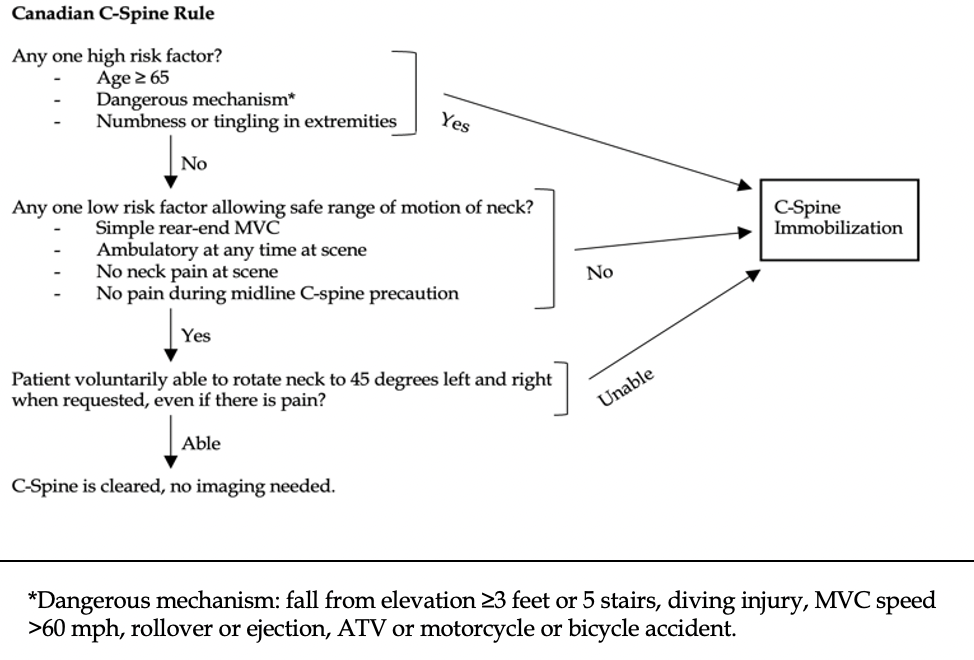
Process: In those with minor trauma, there is usually a lower, but not negligible, risk of cervical spine injury. In these patients, NEXUS or Canadian C-spine Rule should be applied and determine need for cervical spine imaging.
A full neurological exam should be performed in those with a cervical collar prior to clearance.

NEXUS has not been validated in those >60 years old. The Canadian C-Spine mandates CT imaging in those > 65 years old.
Both criteria cannot be used in the following patients: direct blows to neck, penetrating trauma.
Both rules have not been validated in children but are frequently used still as a “guideline” for physicians.
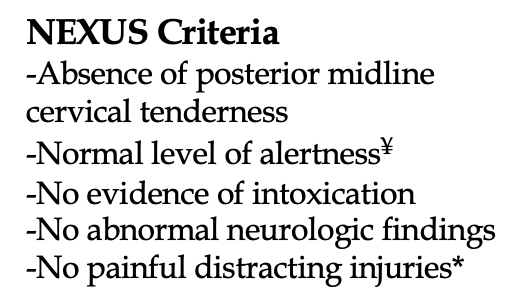
¥ GCS <15, AAO <4, delayed or inappropriate responses to external stimuli. A brief loss of consciousness at the scene does not preclude application of NEXUS.
* Distracting injuries includes long bone fracture, visceral injury requiring surgical consult, large lacerations, crush injuries, large burns.
Negative CT C-spine?
In those with a negative CT C-spine, lack of neck tenderness, and no neurologic deficits on exam, cervical collar may be cleared without specialty consultation or need for MRI.
Spinal cord injury without radiographic abnormality (SCIWORA) is rare but feared. Thankfully, about <1% of patients with SCIWORA require surgical stabilization from an injury found on MRI but CT was negative.
Suspect SCIWORA in those with severe neck pain or upper extremity neurologic deficits. Both the East and West Trauma Guidelines state that negative CT is adequate in the absence of focal neurologic deficits, and persistent midline pain alone is not an indication for MRI. MRI should be performed for these patients when the initial CT C spine is negative.
A negative cervical MRI allows the clinician to clear the C spine at bedside.
References
1. Hanson JA, Blackmore CC, Mann FA, Wilson AJ. Cervical spine injury: a clinical decision rule to identify high-risk patients for helical CT screening. AJR Am J Roentgenol 2000; 174:713.
2. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma. National Emergency X-Radiography Utilization Study Group. N Engl J Med 2000; 343:94.
3. Stiell IG, Clement CM, McKnight RD, et al. The Canadian C-spine rule versus the NEXUS low-risk criteria in patients with trauma. N Engl J Med 2003; 349:2510.
4. Hoffman JR, Wolfson AB, Todd K, Mower WR. Selective cervical spine radiography in blunt trauma: methodology of the National Emergency X-Radiography Utilization Study (NEXUS). Ann Emerg Med 1998; 32:461.
5. Patel MB, Humble SS, Cullinane DC, et al. Cervical spine collar clearance in the obtunded adult blunt trauma patient: a systematic review and practice management guideline from the Eastern Association for the Surgery of Trauma. J Trauma Acute Care Surg 2015; 78:430.
6. Badhiwala JH, Lai CK, Alhazzani W, et al. Cervical spine clearance in obtunded patients after blunt traumatic injury: a systematic review. Ann Intern Med 2015; 162:429.
7. Kirschner J, Seupaul RA. Does computed tomography rule out clinically significant cervical spine injuries in obtunded or intubated blunt trauma patients? [corrected]. Ann Emerg Med 2012; 60:737.
8. Malhotra A, Wu X, Kalra VB, et al. Utility of MRI for cervical spine clearance after blunt traumatic injury: a meta-analysis. Eur Radiol 2017; 27:1148.



